
INFORMATION
What is haemophilia
Haemophilia (from the Greek haima αἷμα ‘blood’ and philia φιλία ‘love’) is a hereditary disease, usually transmitted by the mother. It is much more common in boys than in girls and consists of a predisposition to haemorrhage, caused by the prolongation of blood clotting time. It is a severe haemorrhagic syndrome occurring in male children and is dependant on the transmission of an abnormal gene related to the “X” chromosome. Haemophilia A (factor VIII coagulation deficiency) is the most common form of the disease, present in approximately 1 in 5,000-10,000 male born children. Haemophilia B (factor IX deficiency) occurs in approximately 1 in 20,000-34,000 male newborns

The term haemophilia was first introduced by Schönlein in 1893, although the disease was known since antiquity, described by Rabbi Simon ben Gamaliel in Talmud, by Maimonide (a Jewish physician and philosopher), by Albucasis, an Arab physician (in the 12th century), Addis (1911), Patek and Taylor in 1937 – they demonstrated the presence of an antihaemophilia active factor in normal plasma.
In about half of the cases – haemophilia is a hereditary disease – it is transmitted frogeneration to generation through the female line. And the second half is the result of random genetic mutations. Their secret is still unknown to anyone in the world. This is why in the near future we will not be able to be part of haemophilia. The biggest problem is that these are random, spontaneous mutations. It is impossible to predict them. It is, therefore, impossible to warn.
Haemophilia – symptoms, diagnosis, treatment

Haemophilia is a genetic disease that affects the ability of the blood to coagulate. In other words, haemophilia is a coagulopathy. Typically, haemophilia involves a deficiency of coagulation factors VIII or IX. In people with haemophilia , the bleeding time is extended, depending on how severe the coagulation factor deficiency is.
Haemophillia affects male and only exceptionally female people, in which the forms of illness are much milder..
Causes of haemophilia
Haemophillia is an X-linked genetic disorder, the genes encoding coagulation factors VIII and IX being located on the X chromosome. The mutations of these genes lead to the coagulation disorders encountered in haemophilia.
The defective gene, responsible for the deficiency of coagulation factor VIII or IX, is found on the X chromosome. As we know, females have two X chromosomes in their genetic code. The male ones have an X chromosome and a Y chromosome. If a girl has an X chromosome that carries the gene responsible for haemophilia, she also has a normal X chromosome that will be able to compensate for its pear’s deficiency. Boys, however, having a single X chromosome, have nothing to compensate for its abnormality: the Y chromosome does not have similar properties.
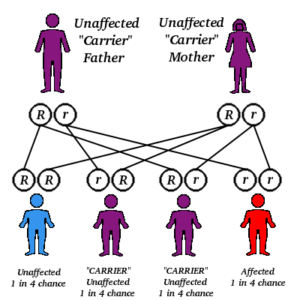
The mother can be a carrier of haemophilia – she has an affected X chromosome. The chances of transmitting the anomaly are 50%.
• The male child has a 50% chance of taking over the X chromosome abnormality from the mother; from his father, it is sure that he took over the Y chromosome (and not the healthy X chromosome) because only this way he could be a boy. With the affected X chromosome taken from the mother, the boy will manifest the disease. The chances for a girl to have haemophilia are rare: both parents must be carriers and pass the affected X chromosomes to the child so that compensation is not possible.
Types of haemophilia
 Haemophillia A, or classic haemophilia , is a factor VIII deficiency. This is the most common type of haemophilia , being 5 times more frequent than haemophilia B. The incidence is 1:10,000 newborns.
Haemophillia A, or classic haemophilia , is a factor VIII deficiency. This is the most common type of haemophilia , being 5 times more frequent than haemophilia B. The incidence is 1:10,000 newborns.
Haemophillia B, or Christmas Disease, is a factor IX deficiency. The incidence is 1:50,000 newborns.
Symptoms of haemophilia
The severity of clinical manifestations depends on the degree of coagulation factor deficiency. Thereby, we may be dealing with mild, moderate or severe forms. If the deficit is severe, the patient may have spontaneous bleeding.
 The characteristic symptom, the one that raises the suspicion of haemophilia , is prolonged bleeding. It can be external, visible as: epistaxis, prolonged bleeding by cutting or scratching, prolonged bleeding from tooth extractions. Most of the time, however, the bleeding is internal, objectifying as hematuria, melena, hematochezia, extensive ecchymosis.Often, the site of spontaneous bleeding or after minimal trauma is represented by the joints, resulting in hemarthrosis. In time, repeated hemarthrosis, due to the irritating effect of blood on the synovial, can cause inflammation and its proliferation, a process that evolves towards haemophilic arthropathy.
The characteristic symptom, the one that raises the suspicion of haemophilia , is prolonged bleeding. It can be external, visible as: epistaxis, prolonged bleeding by cutting or scratching, prolonged bleeding from tooth extractions. Most of the time, however, the bleeding is internal, objectifying as hematuria, melena, hematochezia, extensive ecchymosis.Often, the site of spontaneous bleeding or after minimal trauma is represented by the joints, resulting in hemarthrosis. In time, repeated hemarthrosis, due to the irritating effect of blood on the synovial, can cause inflammation and its proliferation, a process that evolves towards haemophilic arthropathy.
Diagnosis of haemophilia
Very often the manifestations of haemophilia appear from childhood, once the child begins to move on its own. In this case, bruising and bleeding from minor injuries can be noticed. These manifestations raise the suspicion of haemophilia . If there are people in the family with confirmed haemophilia or similar manifestations, the diagnosis is even more likely. In other words, the patient’s history and hereditary-collateral antecedents play a key role, with episodes of prolonged bleeding or intra-articular blood collections guiding the diagnosis.
Being a coagulopathy, modifications of the coagulogram occur. The characteristic of haemophilia is the increased activated partial thromboplastin time (aPTT). Platelet count and prothrombin time are within normal limits.The dosage of coagulation factors in the blood is essential because it establishes the factor that is deficient, so it determines whether haemophilia is type A (factor VIII) or B (factor IX), crucial information for setting up the substitution treatment. It also appreciates the deficit quantitatively, and thus assess the severity of the disease.
Treatment of haemophillia
 The main treatment at present is represented by substitution therapy. In other words, the endogenous deficiency of coagulation factors is compensated by exogenous intake, so that a concentrated solution of factor VIII, forhaemophilia A, or factor IX, for haemophilia B is administered. These factor VIII or IX preparations are injectable and may be of human or synthetic origin.
The main treatment at present is represented by substitution therapy. In other words, the endogenous deficiency of coagulation factors is compensated by exogenous intake, so that a concentrated solution of factor VIII, forhaemophilia A, or factor IX, for haemophilia B is administered. These factor VIII or IX preparations are injectable and may be of human or synthetic origin.
 Substitution treatment can be administered both in case of an acute bleeding episode, to stop the bleeding, but also for prophylactic purposes, in the hospital or at home. The schedule and doses of administration depend on the severity of the disease, in severe forms, it is necessary to administer it throughout the lifetime of the patient. In the case of intra-articular bleeding, blood evacuation is required in order to avoid the development of hemophilic arthropathy. Evacuation puncture may be accompanied by symptomatic treatment, such as analgesic, anti-inflammatory or corticosteroid drugs.
Substitution treatment can be administered both in case of an acute bleeding episode, to stop the bleeding, but also for prophylactic purposes, in the hospital or at home. The schedule and doses of administration depend on the severity of the disease, in severe forms, it is necessary to administer it throughout the lifetime of the patient. In the case of intra-articular bleeding, blood evacuation is required in order to avoid the development of hemophilic arthropathy. Evacuation puncture may be accompanied by symptomatic treatment, such as analgesic, anti-inflammatory or corticosteroid drugs.
 How haemophilia manifests itself
How haemophilia manifests itself
In young children, hematomas often appear on the head, in the area of the buttocks, with shovels. The physiological teeth are accompanied by continuous bleeding. Many times, there is also a discharge of blood from the mucous membranes of the nose and mouth when crushing the tongue and cheeks.
Eye damage is extremely dangerous. Heavy bleeding can lead to complete blindness.
With age, the manifestations become moderate, the bleeding is smoothed, their danger is no longer so great.
 In everyday life, there is a myth of bleeding cases in patients with haemophilia suffering from the slightest excision or scratch. As a matter of fact, it is not like that. Severe surgery and internal bleeding of unexplained origin are dangerous. Most likely, a combination of bleeding mechanisms with diseases and fragility, the permeability of the vascular wall.
In everyday life, there is a myth of bleeding cases in patients with haemophilia suffering from the slightest excision or scratch. As a matter of fact, it is not like that. Severe surgery and internal bleeding of unexplained origin are dangerous. Most likely, a combination of bleeding mechanisms with diseases and fragility, the permeability of the vascular wall.
 Note:
Note:
Recurrent bleeding after an injury has been noticed in patients with haemophilia. On the background of a stop, in a few hours or days, the process can be repeated.
Therefore, it is necessary to carefully monitor such patients. Frequent recurrent bleeding causes anaemia over time.
 |
Motto: “Haemophilia doesn’t wait until morning !” |
Tags
Haemophilia, doctor, blood, coagulation-diagnosis, cromosome-mutation, science-blood, donation, healt-medicine, splashing-person-location, plabelebs, bleed, slimy-bleed-clinical-white, clinic-profesional-suport, disorder, dragstore-medic-condition, red-illnes, job, flow, physician, hemorhage, rhesus-aneamia-splattered-knowledge-help, apothecary, pharmacy-medical, hepatitis, donor-practice, clot, assistant-dripping, platelebs-flowing.